

The Pelvicenter: an innovative medical device dedicated to the pelvic floor
Alternative to traditional perineal rehabilitation methods; the Pelvicenter allows you to strengthen your pelvic floor, without invasive gesture and without pain. A great step forward for caregivers and patients!

Presentation
What is the Pelvicenter?
The Pelvicenter is a DM certified medical device: Class IIa-93/42/EEC Medical Device. It offers a new way of working the pelvic floor, highly effective and non-invasive.
- The Pelvicenter chair produces "pulsed magnetic waves" that trigger regular muscle contractions, ranging from the pelvic floor muscles to peripheral muscle areas.
- Perineal rehabilitation is painless because the action of the magnetic field penetrates the tissues to the motor nerves, but does not act on the sensory fibers.
- The patient is comfortably seated and can keep his clothes on during the session.
For the patient, working in perineal rehabilitation is no longer a painful effort. In some cases, he takes charge of his rehabilitation himself, by controlling the intensity of the impulses.
For the practitioner, the Pelvicenter makes it possible to act effectively, with sessions adapted to each patient. It treats symptoms related to pelvic floor weakness: perineal rehabilitation, stress urinary incontinence, lumbar pain, neurological disorders, etc. for a wide range of patients.
90% of patients with perineal problems and undergoing treatment with the Pelvicenter for perineal reeducation, relaxation, muscle building and strengthening, say they are satisfied. Study carried out between April 2019 & July 2020 by Dr Andrea Muller – Gynecologist, published on Frau Punkt.
Innovative and efficient
How does the Pelvicenter work?
The Pelvicenter is a medical device using OMP: “pulsed magnetic waves”. These trigger regular muscle contractions of the pelvic floor muscles and peripheral muscle areas.
The patient is seated, fully clothed, on the device. An electromagnetic coil in the seat cushion generates pulsed magnetic fields. They penetrate the tissues up to the motor nerves but do not reach the sensory fibers which have a narrower diameter. Hence a painless stimulation and perineal re-education without constraint for the patient.
The magnetic field acts:
- Directly on the motor nerve, causing muscle contraction by sensorimotor pathway
- Indirectly, by stimulating the mechanoreceptors through the rhythmicity of muscle contractions
The effectiveness of the treatment is therefore the result of a double action:
- On the one hand, a remusculation and retonification, deep and global of the muscles of the pelvic floor by the powerful contractions caused by the device.
- On the other hand, an action on the cortical representation of the pelvic floor induced by the stimulation of mechanoreceptors. This improves proprioception and control of voluntary contraction of the pelvic muscles.

What are the possible fields of application?
The Pelvicenter is a new powerful approach to perform perineal rehabilitation, but it also concerns a large number of pathologies.
Many professionals and health establishments use it to painlessly treat pelvic disorders in women and men:
- Gynecologists – Obstetricians
- Urologists
- Midwives
- Physiotherapists
- Gastroenterologists, proctologists
- Digestive surgeons
- Physiotherapists
- General practitioners
- Care centers
- Rehabilitation centers
- Clinics and hospitals
- EHPAD
INCONTINENCE
- In women: postpartum perineal rehabilitation, stress urinary incontinence, urgency, etc.
- In men: especially after a prostatectomy or for incontinence problems
- Fecal incontinence
PREVENTION
- Before a prostatectomy
- Before or after a cure for genitourinary prolapse (organ descent)
- In the event of significant solicitation of the pelvic floor, particularly in high-level athletes
BACK PAIN
- Especially for lower back pain and pain in the lumbar vertebrae
NEUROLOGICAL DISORDERS
- Neurological bladder, neuralgia (pudendal neuropathy)
- Enuresis in children and adults


The commissioning of the Pelvicenter is done with our medical and technical director, Dominique Trouillet. Each practitioner receives a one-day theoretical and practical training, which allows him to master all the parameters of use. Following which we award a diploma.
A recognized medical device
How is the installation of a Pelvicenter carried out?
The Pelvicenter is installed on a flat surface away from any heat source and should not be moved. It is plugged into the mains (230 V – 50 Hz).
The device works with a computer program and smart cards (one per patient). The practitioner individually programs the treatment of each patient from his computer (intensity, frequency, duration of the session, position of the coil, etc.). At the start of the session, he inserts the smart card into the slot of the Pelvicenter and checks the information on the control panel. The treatment can then begin for a period of 15 minutes.
Pelvicore accompanies each installation and ensures that the practitioner understands how to use the Pelvicenter. Commissioning, settings, functions, patient preparation are discussed during theoretical and practical training. It is the guarantee for the practitioner, of an installation and use, in all serenity and efficiency.
In order to check all the functions, it is recommended to carry out one maintenance operation per year. Inspection and maintenance are carried out by us or by an approved Pelvicore agent. To find out more, contact us on 210.389.7332.
A recognized medical device
The advantages of a treatment with the Pelvicenter
- The treatment achieves better results than conventional methods
- The treatment is non-invasive (the patient remains dressed, no probe)
- The patient does not provide any physical effort and performs his session independently.
- The duration of a session is only 15 minutes. Depending on the pathology treated, 8 to 36 sessions are necessary.

- The practitioner adapts the treatment and the intensity of the sessions to each patient.
- Muscle building is effective and lasting
- Incontinence problems are reduced, sexual sensitivity improves, back pain disappears, muscle replaces cellulite.




Muscle training for a strong pelvic floor
The QRS 1010 Pelvicenter — a.k.a. the magnetic chair — is a non-invasive form of pelvic floor treatment that aims to restore and strengthen the pelvic floor muscles. The patient is not required to participate actively in muscle training.
The family of procedures is known as PMS (pulsed magnetic stimulation) or RPMS (repetitive peripheral magnetic stimulation). When used to treat the pelvic floor, the PMS procedure is known as TPM (transpelvic magnetic stimulation). High-intensity, pulsed signals are used to control the muscles in the pelvic floor and the adjacent body core and thigh muscles. The muscle fibres are rhythmically contracted and relaxed without any conscious effort by the patient.


Description of the procedure
The effects of QRS Pelvicenter technology are comparable to those induced by TENS/EMS. But PMS, i.e. RPMS, is a substantially more complex procedure from a technical perspective. The induction of current flow through the nerves that control the muscles causes the muscles to contract. The benefits compared to electrical nerve stimulation are firstly that the procedure does not cause painful sensitivity of the skin and secondly that the biological field of action of the Pelvicenter penetrates far deeper into the tissue.
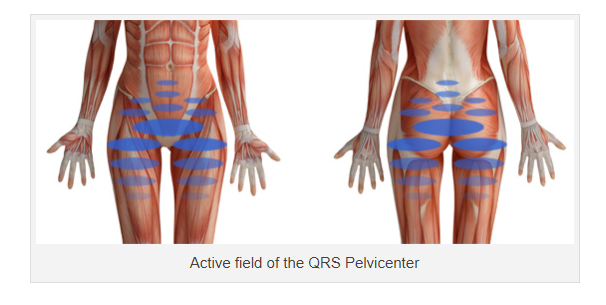
The following diagram shows the extent of the field of action when the Pelvicenter is running at 60% device output. The effective penetration depth at 60% device output is approx. 120 mm. At higher settings, the effective penetration depth rises to as much as 150 mm. The breadth of stimulation is approx. 400 mm at 100% device output.

The pelvic floor muscles are contracted several thousand times during a 15 to 20-minute therapy session on the QRS Pelvicenter. Hence, the effects of pelvic floor training with the Pelvicenter are incomparably higher than even the best possible results of classic pelvic floor training. A more effective and simultaneously more comfortable therapeutic procedure than Pelvicenter muscle stimulation to reactivate weakened pelvic floor muscles simply does not exist.
Who Is the patient?
Potential patients include women who have recently given birth and are determined to reduce susceptibility to urinary incontinence later in life, as well as older women with bladder weakness who refused to undergo invasive urological surgery or for whom more traditional measures are more difficult to implement.
RPMS is also suitable for patients experiencing urinary incontinence after a radical prostatectomy. Erectile dysfunction is another important application area. Most cases of erectile dysfunction are caused by impaired venous drainage or by reorganisation processes in the cavemous bodies of the penis (fibrosation). RPMS therapy provides a transparent treatment model in both cases.

Comparison with classic pelvic floor training
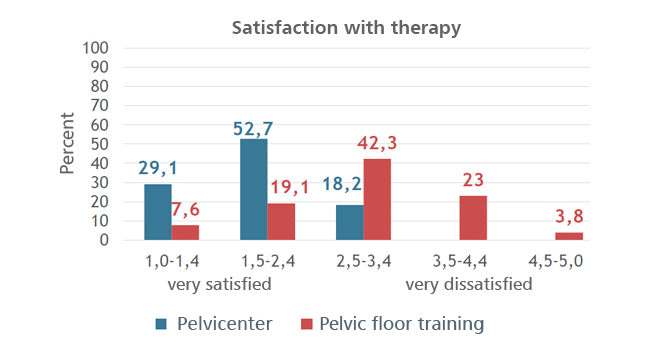
The University of Vienna conducted a study (Aug. 2015) with 73 Nursing home residents to compare Pelvicenter training with classic pelvic floor training. 39 people took part in the pelvic floor training, while 42 were included in the Pelvicenter group. The forms of urinary incontinence were mixed incontinence and stress incontinence; the average age was approximately 80
Besides the therapy outcome, subjective perceptions of both therapy methods were also compared. The conclusions drawn by the study organiser indicate that classic pelvic floor training, applied in a consistent form with expert guidance, can achieve outcomes that are similar to technology-assisted therapy using the Pelvicenter. “Overall, however, it is evident that pelvic floor training is only suitable for a small proportion of residents in long-term care facilities, while Pelvicenter training is a conceivable and feasible form of treatment for persons with both mobility restrictions and cognitive impairments. In consequence, a significantly larger number of older citizens would receive access to appropriate and effective incontinence therapy.”
The results of the aforementioned study reflect the outcomes of all other studies and observations on this subject. The Pelvicenter group is significantly more satisfied with therapy than is the pelvic floor training group. Pelvicenter: Alleviation of urinary incontinence symptoms; significant reduction in the urge to urinate; improvement in individual well-being Pelvic floor training: difficult to apply independently; moderate therapeutic success.
Additional beneficial effects
The Pelvicenter affects the whole body core. Therefore, not only does the therapy train the pelvic floor muscles, it also activates the muscles in the lower abdomen and back, the buttocks, thighs and the (dorsal) layer of the rear hip muscles. Physical exercise is the only other way of achieving these effects. Pelvicenter training therefore has an extremely positive influence on the entire coordination of the supporting apparatus.
Frequency settings above 35 Hz release adhered fascia, above all in the lumbar region (loin area) as well as in the gluteus maximus and medius (lumbago muscles). The high frequencies can even counteract muscle hardening and trapped nerves within the field of action.
Benefits for the operator
In many cases it is difficult to conduct classic pelvic floor training with the patient. It is common to encounter patients displaying a reluctance to cooperate or poor discipline when attempting to comply with the prescribed training regime in home settings.
The QRS Pelvicenter radically changes this situation. The attending physician or therapist can directly control therapeutic success, instead of being forced to rely on unpredictable patient discipline or willingness to comply.
Benefits for the patient
The patient takes a seat in the QRS Pelvicenter and can feel the muscles working without experiencing any pain. The patient is not required to do anything. In this way they can do nothing wrong. Patients are not required to undress, and can complete the therapy sessions in their everyday clothes.
Predictable duration of treatment
2-3 therapy sessions of 15-20 minutes are recommended per week. A positive therapy outcome requires 10 to 20 treatments. But the targeted medical strengthening therapy of the pelvic floor musculature ensures that many patients observe a noticeable alleviation of symptoms after just a few sessions.
Prospects of success
Trials and observation studies have demonstrated extremely high patient satisfaction, in addition to an excellent responder result. Assuming the problems are caused by weakened pelvic floor muscles, it is reasonable to assume that a significant improvement or complete alleviation of symptoms will occur.
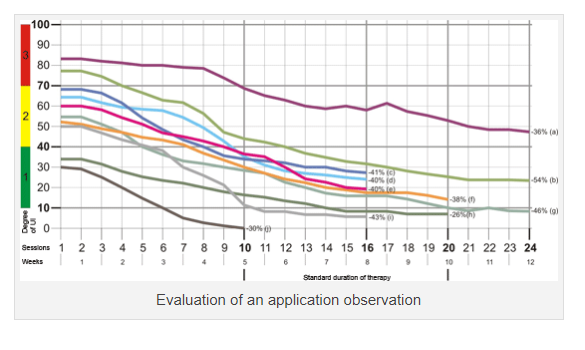
The analytical data was provided by commercial Pelvicenter users in a variety of countries. The average age was 58.5, and all the individuals studied were female. The indication in all cases was stress incontinence. The therapeutic frequency was 3 sessions per week. The duration of therapy was 10 sessions in one case, 16 sessions in four cases, 20 sessions in two cases and 24 sessions in three cases. A reduction in UI severity by at least one grade was achieved for all patients. Therapeutic success and progress were higher in the first 10 to 16 sessions than in the following treatments.
Available data
The available data is unequivocal with regard to the treatment of urinary incontinence. The mean success rate is approximately 70%. There are currently three studies available, in addition to our own observation studies.
For an overview of the studies, visit the page >Research >Studies. We will gladly send you a copy of the original study upon request. To obtain your copy, send an email to info@ThePelvicenter.com and enclose legitimisation credentials with your message.
Expert Advice
Are you interested in The Pelvicenter?
We are happy to provide you with expert personalized advice.Do not hesitate to contact us.
info@ThePelvicenter.com
Phone : 210.389.7332